BY: SAI MANOGNA (MSIWM014)
Introduction :
Mycobacterium tuberculosis, a tubercle bacillus, is the TB causative agent. It belongs to a closely related species, including M bovis, M africanum, and M microti, in the M tuberculosis complex. The most common site for TB development is in the lungs; 85 percent of patients with TB have lung complaints. Extrapulmonary TB can emerge as part of a primary, or late, generalized infection.
Types of Tuberculosis :
Tuberculosis is categorized into two types: active illness or latent infection. Lung disease is the most common type of active TB, but it can invade other organs, known as “miliary TB.”
TB – Active :
Active TB is a disease in which TB bacteria rapidly grow and invade the body’s various organs. Cough, phlegm, chest pain, fatigue, weight loss, fever, chills, and night sweating are common symptoms of active TB. Via airborne transmission of infectious particles coughed up into the air, a person with active pulmonary TB disease may spread TB to others.
TB Miliary :
Miliary TB is a rare type of active disease in the bloodstream when TB bacteria find their way. The bacteria rapidly spread across the body in tiny nodules in this form, affecting multiple organs at once. This form of TB can quickly become fatal.
Latent Infection with TB :
Many of those infected with TB may not experience overt illness. They have no symptoms, and that could be common for their chest x-ray. Reaction to the interferon-gamma release assay (IGRA) or tuberculin skin test (TST) may be the sole manifestation of this encounter. There is an ongoing possibility, however, that the latent infection can escalate to active illness. Other diseases, such as HIV or drugs that weaken the immune system, increase the risk.
Incubation Period :
The time of incubation can vary from two to 12 weeks or so. An individual may remain infectious for a long time (provided that viable TB bacteria are present in the sputum) and may remain infectious for several weeks before they have undergone sufficient therapy.
Pathophysiology :
1. M tuberculosis infection occurs most often from exposure to infected aerosols from the lungs or mucous membranes.
2. Droplets are 1-5 μm in diameter in these aerosols; a single cough will produce 3000 infectious droplets in a person with active pulmonary TB, with as few as 10 bacilli required to initiate infection. Droplet nuclei are deposited within the terminal airspace of the lung when inhaled.
3. The organism will grow for 2-12 weeks until they reach several 1000-10,000, enough to evoke a cellular immune response, detected by a tuberculin skin test reaction.
4. Mycobacteria are strongly antigenic and encourage a nonspecific immune response that is robust.
5. Their antigenicity is due to the activation of Langerhans cells, lymphocytes, and polymorphonuclear leukocytes by multiple cell wall constituents, including phospholipids, glycoproteins, and wax D.

Individuals infected with M tuberculosis may take 1 of several infection routes, most of which do not lead to actual TB. The host immune system can clear or suppress infection in an inactive type called latent tuberculosis infection (LTBI), with resistant hosts regulating mycobacterial production at distant locations before active disease output. Patients with LTBI cannot spread TB.
As earlier mentioned, the most popular site for TB production is in the lungs; 85 percent of TB patients have pulmonary complaints. As part of primary infection, or late, generalized infection, extrapulmonary TB may occur. The most prominent sites of extrapulmonary disease are: common location of tuberculous lymphadenitis is in the neck and the sternocleidomastoid muscle; it is typically unilateral and causes little to no pain; advanced tuberculous lymphadenitis cases may suppurate and shape a sinus drain. As in the kidneys, bones, meninges, skin, choroids, and the lungs’ apices, contaminated end organs usually have high regional oxygen stress. The fundamental cause of M tuberculosis infection tissue destruction is linked to the organism’s ability to incite extreme host immune reactions to the antigenic cell wall proteins.
Lesions with TB :
An epithelioid granuloma with central caseation necrosis is the usual lesion of TB. The common site of the primary lesion in the lung’s subpleural regions is within alveolar macrophages. Locally, Bacilli proliferate and spread to a Hillary node via the lymphatics, forming the Ghon complex.
The early tubers are spherical, 0.5- to 3-mm nodules with 3 or 4 cell areas, displaying the following characteristics:
a. A necrosis of the central caseate
b. Lymphocyte-admixed inner cell region of epithelioid macrophages and Langhans giant cells
c. An outer cell region with plasma cells, lymphocytes, and immature macrophages
d. A fibrosis rim (in lesions that heal)
Initial Lesions: Until symptomatic illness occurs, initial lesions may heal, and the infection becomes latent. Smaller tubercles can be fully resolved. Fibrosis happens when hydrolytic enzymes destroy tubercles, and a fibrous capsule surrounds larger lesions. Typically, these nodules contain viable mycobacteria and can be reactivated. Some nodules calcify or ossify and are readily seen on radiographs of the chest.
Proliferative Lesions: Where the bacillary load is small and host cellular immune responses dominate proliferative lesions form. These tubers are compact, mixed with activated macrophages, and surrounded by proliferating fibrosis lymphocytes, plasma cells, and an outer rim. Mycobacteria intracellular killing is successful, and the bacillary load remains low.
Exudative Lesions: Exudative lesions predominate when large numbers of bacilli and there are low host defenses. Such loose aggregates of immature macrophages, neutrophils, necrosis of fibrin, and caseation are mycobacterial growth sites. These lesions progress without treatment, and the infection spreads.
Etiology :
M tuberculosis, a slow-growing obligate aerobic and a facultative intracellular parasite, are responsible for TB. In parallel groups called cords, the organism grows. After decoloration with acid-alcohol, based on the acid-fast stains used for pathological detection, it retains several stains.

Fig: Acid-fast bacillus smear.
In Mycobacterium tuberculosis, acid-fast bacillus smear shows aerobic, non-spore-forming, nonmotile, facultative, curved intracellular rods measuring 0.2-0.5 μm by 2-4 μm are mycobacteria, including M tuberculosis. Mycolic, acid-rich, long-chain glycolipids and phospho lipoglycans (mycocides) are contained in their cell walls that protect mycobacteria from cell lysosomal attack retains red basic fuchsin dye (acid-fast stain) after acid rinsing.
Transmission :
The only known source of M tuberculosis has been humans. The organism is transmitted from a person in the infectious stage of TB, primarily airborne aerosol (although transdermal and GI transmission have been reported).
1. Exposure to M tuberculosis in immunocompetent individuals results in latent/dormant infection
2. Modifications in host immune systems resulting in a decreasing immune effectiveness may enable M tuberculosis species to reactivate, tuberculosis stemming from a combination of the direct effects of infectious organism replications, and subsequent host immune responses to tuberculosis antigens.
3. By restriction fragment-length polymorphism study, molecular typing of M tuberculosis isolates in the United States indicates that more than one-third of new patient TB occurrences result from person-to-person transmission. The remainder comes from latent infection reactivation.
Symptoms and signs :
Symptoms associated with active pulmonary TB (older people with TB do not have the usual signs and symptoms) are as follows:
i. Coughing ii. anorexia and fever
iii. Sweats at Night
iv. hemoptysis
v. Chest pain (may also be caused by acute tuberculous pericarditis)
vi. Tiredness
The following may be signs of tuberculous meningitis:
i. Headache, which for 2-3 weeks has been either sporadic or chronic
ii. Fever that is low-grade or absent
iii. Subtle changes in mental state that may progress towards coma over days to weeks
The following may be signs of skeletal TB :
i. Pain in the back or stiffness
ii. Tuberculous arthritis, usually affecting just 1 joint (the hip or knee most frequently, followed by the foot, elbow, wrist, and shoulder)
Genitourinary TB symptoms can include the following:
Pain Flanking, DYSURIA, frequent urination, symptoms that resemble pelvic inflammatory illness in women, a painful mass of the scrotum, prostatitis, orchitis, or epididymitis in men
Gastrointestinal TB signs apply to the contaminated site and can include the following:
i. Non Healing mouth ulcers or anus ulcers
ii. Malabsorption (with a small intestine infection)
iii. Swallowing problems (with the esophageal disease)
iv. TB-related physical examination results depend on the organs involved.
v. Mimicking peptic ulcer disease (with gastric or duodenal infection) with stomach pain
vi. Pain, diarrhea, or hematochezia (containing colon infection)
The following may be present in patients with pulmonary TB:
i. Abnormal sounds of breath, especially over the upper lobes or areas involved,
ii. Rales or signs of bronchial breath, suggesting consolidation of the lungs
Depending on the tissues involved, symptoms of extrapulmonary TB vary and can include the following: Perplexity, chorioretinitis, coma, cutaneous Injuries, neurological deficit, lymphadenopathy pathology.
Active TB is not excluded by the lack of any relevant physical findings. In high-risk patients, especially those who are immunocompromised or elderly, classic symptoms are often absent.
Causes :
M. Bacteria that cause tuberculosis to induce TB. When a person with pulmonary TB coughs, sneezes, spits, laughs or speaks, they will propagate in droplets through the air. The infection can be transmitted only by individuals with active TB. However, most people with the disease can no longer spread the bacteria after receiving sufficient care for at least two weeks.
Factors of Risk :
When deciding whether a TB infection is likely to be transmitted, the following factors help:
i. Total of expelled species
ii. Immune condition of the person exposed
iii. Duration of time of exposure to polluted air
iv. Organisms’ concentration
A specific risk to non-infected individuals is posed by infected persons living in crowded or closed environments. Approximately 20% (positive tuberculin skin test) of household contacts develop an infection. Micro Epidemics have occurred on transcontinental flights and in closed settings such as submarines. Hospital workers, inner-city residents, nursing home residents, and inmates often include groups at high risk for contracting the infection.
The factors increasing the risk of acquiring active tuberculosis in an individual are :
i. Infection with HIV
ii. Diabetes mellitus (3fold increase in risk)
iii. Immunosuppressive counseling
iv. Abuse of intravenous ( IV) medications
v. Renal End-stage Disorder
vi. With alcoholism
vii. Malignancies of hematologic origin
viii. Silicosis
ix. Less than five years of age
x. Antagonists of tumor necrosis factor-alpha (TNF-alp)
xi. Head and neck cancer
xii. Surgery for intestinal bypass or gastrectomy
xiii. Chronic Syndromes of Malabsorption
xiv. Low body weight-In comparison, obesity has been associated with a lower risk of active pulmonary TB in elderly patients
xv. Smoking-To minimizes the risk of relapse; smokers who develop TB should be advised to quit smoking.
TB in Children :
The potential for developing fatal miliary TB or meningeal TB is a primary concern in children younger than five years old. In children with TB, osteoporosis, sclerosis, and bone involvement are more common than adults with the condition. As a result of their high vascularity, the epiphyseal bones may be involved. Children also do not infect other children because they rarely develop a cough, and sputum development is scarce. Cases of child-child and child-adult transmission of TB are, however, well known.
Genetic considerations :
Tuberculosis genetics are very complex, involving several genes. Some of these genes provide essential elements of the immune system, while others include more complex mechanisms by which Mycobacterium species communicate with the human body. The genes that follow have polymorphisms that are connected with either tuberculosis susceptibility or safety. Also, regions such as 8q12-q13, the gene has not yet been identified, are associated with increased risk.
Diagnosis :
Methods of screening for TB include:
Mantoux tuberculin skin test for active or latent infection (primary method) with purified protein derivative (PPD)
An interferon-gamma release assay (IGRA) in vitro blood test with antigens unique to Mycobacterium tuberculosis for latent infection
Obtain the following laboratory examinations for suspected TB patients:
Acid-fast bacilli (AFB) smear and sputum culture obtained from the patient: no positive smear result does not preclude active TB infection; the most specific test for TB culture is the AFB culture.
Serology of HIV in all TB patients and uncertain HIV status: HIV-infected individuals are at increased risk of TB
Other diagnostic tests, including the following, can justify consideration:
Immunospot Specific Enzyme-Linked (ELISpot)
Tests for Nucleic acid amplification
Community of blood
Drug susceptibility testing should be followed in supportive cultures; symptoms and radiographic results do not distinguish multidrug-resistant TB (MDR-TB) from completely susceptible TB.
Such testing can include the following:
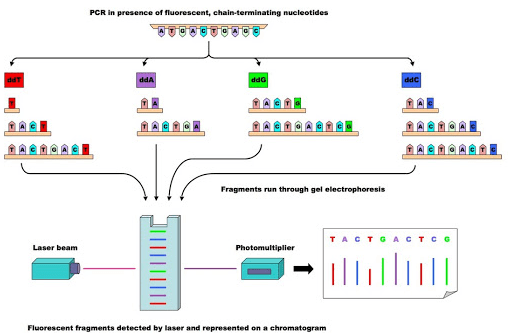
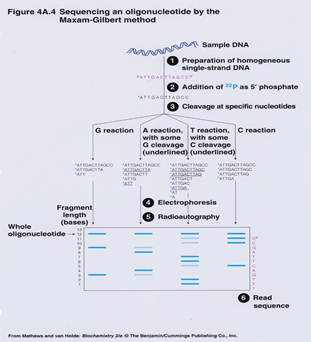
a. Study of Direct DNA Sequencing
b. Molecular Automated Testing
c. Drug resistance (MODS) and thin-layer agar (TLA) assays for microscopic observation
d. Additional quick tests (e.g., BACTEC-460, luciferase reporter assays, ligase chain reaction, FASTPlaque TB-RIF)
e. To test for potential related pulmonary findings, obtain a chest radiograph.
Treatment :
TB is cured with early detection and effective antibiotics.
The correct type of antibiotic and the period of therapy will depend on:
i. The overall health and age of the individual
ii. If they have active or latent TB
iii. The position of the infection
iv. If the TB strain is immune to drugs
v. Latent TB treatment can vary. It may mean taking an antibiotic for 12 weeks once a week or for nine months every day.
Treatment for active TB can require 6-9 months of taking several drugs. The treatment would be more difficult if a person has a drug-resistant strain of TB. Completing the full course of treatment is significant, even if the symptoms go away. Some bacteria can survive and become immune to antibiotics if a person stops taking their medication early. The person may continue to develop drug-resistant TB in this case.
Prevention: Ways of preventing anyone from being infected with TB include:
i. Having an early diagnosis and treatment
ii. Staying away from other individuals until the risk of infection is no longer present
iii. Wearing a mask, shielding the mouth and rooms with ventilation
iv. Vaccinating against TB
In individual nations, as part of a routine immunization program, children receive an anti-TB injection, the bacillus Calmette-Guérin ( BCG) vaccine.
The live strain of Mycobacterium bovis developed by Calmette and Guérin for use as an attenuated vaccine to prevent tuberculosis ( TB) and other mycobacterial infections is Bacille Calmette-Guérin (BCG). The vaccine was first given to humans in 1921 and remained the only vaccine for general use against TB.
The BCG vaccine is the world’s most commonly administered vaccine; it has been given to over three billion people, mainly in the form of compulsory newborn immunization (as dictated by World Health Organization guidelines)[1]. Several BCG vaccines are used worldwide, manufactured by various manufacturers, and administered under different schedules. The BCG vaccine is also effective against other diseases, including leprosy and Buruli ulcer, for safety. Moreover, it is used in the treatment of superficial bladder carcinoma as an immunostimulant.